







 Vishy Iyer, professor of biology, and Matt Cowperthwaite, research director of St. David's NeuroTexas Institute. Photo by Alex Wang
Vishy Iyer, professor of biology, and Matt Cowperthwaite, research director of St. David's NeuroTexas Institute. Photo by Alex Wang
When patients are diagnosed with glioblastoma, one of the worst forms of brain cancer, their options are limited.
Even after surgically accessing the brain to remove as much of the tumor as possible and applying intense chemotherapy, the prognosis is poor. The average survival time is about 14 months. “There are really no good treatments,” said Vishy Iyer, a professor of molecular genetics and microbiology in the College of Natural Sciences at The University of Texas at Austin, who is trying to change that. “You can do surgery and chemotherapy, but glioblastoma is just bad to have.”
Symptoms can start as headaches and nausea. If ignored, the tumor continues to grow, putting pressure on other parts of the brain. Seizures appear. As the tumor’s size increases further, the pressure in the skull becomes life threatening as even far reaches of the brain are bruised against the skull. This begins the progressive deterioration of personality and memory.
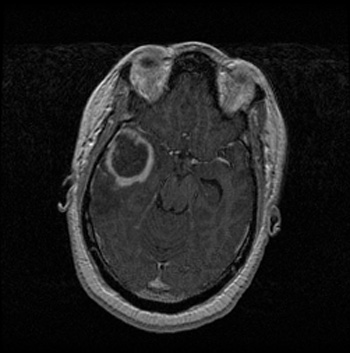 A magnetic resonance (MR) image reveals a lesion (the circular object with a dark center in the upper left portion) from a patient with glioblastoma multiforme, the most common and most deadly form of primary brain tumor in adults. Image courtesy of NeuroTexas Institute.Before surgery — even before symptoms appear — a cancerous tumor starts as what can only be considered a freak accident: a mutation, a random change in a cell’s DNA that leads to uncontrolled cell division. Different mutations cause different cancers and even different molecular subtypes of cancers.
A magnetic resonance (MR) image reveals a lesion (the circular object with a dark center in the upper left portion) from a patient with glioblastoma multiforme, the most common and most deadly form of primary brain tumor in adults. Image courtesy of NeuroTexas Institute.Before surgery — even before symptoms appear — a cancerous tumor starts as what can only be considered a freak accident: a mutation, a random change in a cell’s DNA that leads to uncontrolled cell division. Different mutations cause different cancers and even different molecular subtypes of cancers.
Using these mutations to classify subtypes could lead to better, more personalized treatments for glioblastoma. That’s what Iyer — in collaboration with Matt Cowperthwaite, director of research at the NeuroTexas Institute at St. David’s HealthCare — is hoping to be able to do.
Iyer and Cowperthwaite are taking advantage of two resources: the Austin Brain Tumor Repository started by Cowperthwaite and a technology known as next-generation, or “next-gen,” sequencing.
“Compare making an old-fashioned, smudged fingerprint with ink to making fingerprints with a high-resolution, digital scanner,” Iyer said. “The results we can now obtain, thanks to next-gen sequencing, can be very powerful and very exciting.”
DNA sequencing is the process by which scientists determine the order of the nucleotide bases — thymine, adenine, guanine, cytosine — in a piece of DNA. Next-generation sequencing, a concept first developed in 2004, provides a way to perform this task more quickly and less expensively.
Conventional sequencing processes can process DNA at approximately 100,000 bases per day with a cost of about 5 cents per base. Iyer’s group uses the next-generation sequencing techniques to sequence roughly 1 billion bases per day at about 0.00002 cents per base.
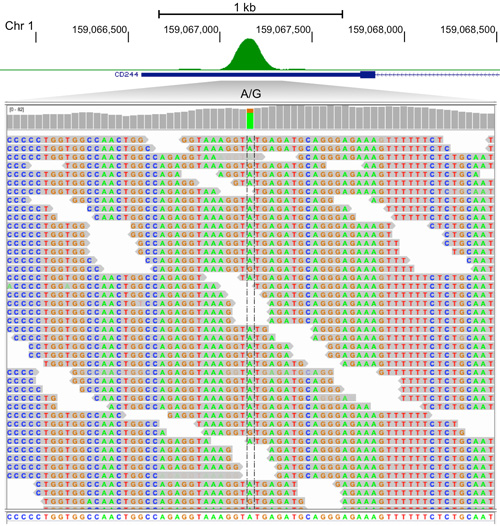 A genetic sequence of part of a glioblastoma tumor cell's DNA. The researchers' goal is to understand how the genetic control sequences vary between glioblastoma tumors. Image courtesy Vishy Iyer.What this sequencing will allow them to do, said Cowperthwaite, is get a better insight into the individuality of tumors.
A genetic sequence of part of a glioblastoma tumor cell's DNA. The researchers' goal is to understand how the genetic control sequences vary between glioblastoma tumors. Image courtesy Vishy Iyer.What this sequencing will allow them to do, said Cowperthwaite, is get a better insight into the individuality of tumors.
“You and I could both have the same type of tumor, in the sense that the clinical diagnosis may be glioblastoma, but yours may be different from mine,” he added. “And I feel as if this research will lead to a better understanding of what is driving those differences.”
The researchers believe that a source of these differences may be mutations in or around molecules known as transcription factors.
“Transcription factors are switches,” Cowperthwaite said. “Essentially they are like light switches; they turn genes on and off. They typically only control particular light switches. But, as the tumors accumulate mutations and change, they may learn how to turn on new lights, or they may lose the ability to turn on or off some lights they normally control.”
To identify these mutations Iyer is using a technique that can essentially identify and isolate what part of the DNA the transcription factors associate with. That DNA is then sequenced specifically in search of mutations.
“Our project is taking a unique approach by focusing on the cancer’s regulatory pathways and the DNA mutations that take place inside the tumor’s regulatory pathways instead of sequencing the entire genome of the cancer like many researchers are currently doing,” Iyer said.
The project uses a sort of double comparison. Iyer and Cowperthwaite have access to both tumor sample DNA and blood sample DNA for each patient. First, they compare these two samples to see what mutations are unique to each tumor.
Then, because Cowperthwaite has given Iyer access to many glioblastoma samples, they plan to compare the mutations against those in all of the other tumors using sophisticated computing software.
Cowperthwaite started the Austin Brain Tumor Repository in 2011. He and his team work closely with neurosurgeons and neuroncologists to learn of tumor operations taking place at the hospital.
“Normally, most of the tumor tissues that are removed during surgery are discarded as biowaste,” he said, adding that besides the initial purchase of a powerful freezer, the tumor bank has been relatively inexpensive to maintain. “When we learn of an operation, we go in and ask the patient if they would want to donate their tumor tissue to research. The vast majority says it’s an easy decision.”
Determining the patterns of different mutations in different tumors will allow the team to identify molecular subtypes of the cancer. The hope of the researchers is that this information can one day be used to develop personalized therapies for cancer.
“Instead of a treatment like chemotherapy that hits all dividing cells, we may be able to use drugs that target specific types of subtypes of tumors,” Iyer said. “Identifying different subtypes based on different interrupted regulatory pathways will allow for the use of specific drugs that interact with specific pathways.”
Although Iyer and Cowperthwaite are still trying to identify the molecular subtypes of glioblastoma and years of more research would be needed to produce these specific drugs, there are several possibilities for treatment if the dream is realized.
If the cancer is caught in an early stage, its growth could be halted by disrupting the specific pathways that keep it dividing and functioning. At later stages there is the possibility of removing a large part of the tumor and then stopping the growth of what remains. This could result in permanent remission.
“Cancer is moving out of this phase of just finding the changes that caused the tumor, which we were doing just five years ago,” Cowperthwaite said. “Inventories of mutations are interesting catalogs, but translating that into something that is actionable is becoming more prominent. That movement is what Vishy and I want to be a part of. Perhaps someday we will be able to run detailed genetic tests on a patient’s tumor and say, ‘Here's a treatment plan that will cure your disease.’ ”









Comments 1
My son, John william Warren died of a glioblastoma brain tumor 8 years ago at age 43. His first glioblastoma occured when he was 22 and a senior at Texas A&M. His tumor then was deep in the brain, in the "zipper" between the left and right side of the brain. It was also in "lay terms" used by the doctors "the size of a peach." I have written a book about his miraculous survival for 2o years afther the removal of the first tumor (astrocytoma grade 3). In the book I quote directly from many medical records from the first tumor and the second tumor 20 years later - records that I saved. His fist "symptoms" in retrospect started when he was 15 - that too is reported in the book with a note quoted from the doctor who treated him then and the note giving his diagnosis at that point in time. What I did not write about in the book was the fact that in 1960 my "obgyn" prescribed and I took a medication when I was within the first 6 weeks of preganancy to prevent miscarriage because I had spotted and was threatening miscarriage. I would have never given that medication that any further thought had John not had the brain tumor. I know of no family history of brain tumors, and otherwise John was a healthy child and adult. I can't help but beleive that the medication given was in some way related to gene mutation which led to his brain tumor. If you would like a copy of the book which includes the medical records that I saved through the years, I will send it to you. I also established a modest brain tumor research fund in his memory at TAMU Health Science Center. I hope that your research will lead to a cure for this deadly and tragic desease that to me (from my own unscientific observation) seems to be on the rise. My son John also hoped that someway his participation in clinical trials following the second tumor, etc at MDA would lead to cures, giving meaning to his suffering and death. Sara Jane White, PhD